Rapid Maastricht type 3 donors and normothermic perfusion: Relieving time constraints in non-renal organ recovery
Brianna Ruch1, Kayla Kumm1, Wendy Van Kirk2, PJ Geraghty2, Jack W Harbell1, Bashar A Aqel3, Kunam S Reddy1, Nitin N Katariya1, Amit K Mathur1.
1Transplant Surgery, Mayo Clinic Arizona, Phoenix, AZ, United States; 2Donor Network of Arizona, Tempe, AZ, United States; 3Transplant Hepatology, Mayo Clinic Arizona, Phoenix, AZ, United States
Purpose: Donation after circulatory death (DCD) liver allografts require short cold ischemia times (CIT) to minimize recipient complications. Historically, these CIT limitations have precluded liver utilization from DCD donors whose infectious disease testing (IDT) were not resulted by time of procurement. Normothermic machine perfusion (NMP) of the liver reduces graft implantation urgency and allows for a grace period of up to 24 hours. We present several cases of rapid Maastricht Type 3 DCD donor offers where NMP was used to allow time for IDT finalization, organ allocation and recipient selection.
Methods: Four rapid DCD donors were pursued by our single, large volume center. Rapid donors were expedited secondary to medical instability or family constraints. In all cases, IDT had not resulted by the time of procurement. All procurements were performed by our own surgical team and the livers placed on the NMP device (TransMedics ™ OCS). The livers were pumped until IDT resulted and were satisfactory. The liver allografts were then successfully transplanted into appropriate recipients.
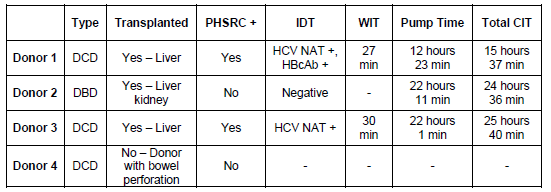
Results: Of the four DCD donors pursued, one donor progressed but the organ was determined non-transplantable. One of the DCD donors was declared brain dead immediately prior to donation and was procured as a DBD. Two of the four donors did meet PHS risk criteria (PHSRC +). A total of 3 liver grafts were procured, placed on the TransMedics ™ OCS device and pumped between 12 to 22 hours until final IDT resulted. Two donors’ final IDT were positive for HCV NAT and one for HBcAb. No prohibitive IDT resulted, and all three livers were then transplanted per our protocol. A donor summary is summarized in Table 1. All liver recipients had satisfactory graft function and are doing well at a minimum follow up of 1 month.
Conclusion: Rapid Maastricht type 3 donors are increasingly more common as DCD donation grows. With well-coordinated logistics and quickly accessible organ recovery, these donors can provide a valuable source of non-renal organs. In donor situations with unyielding time constraints, NMP liver perfusion provides a durable temporizing solution for IDT finalization, organ allocation and recipient logistics.
Lectures by Kayla R Kumm
| When | Session | Talk Title | Room |
|---|---|---|---|
|
Thu-19 13:00 - 14:00 |
DCD | Rapid Maastricht type 3 donors and normothermic perfusion: Relieving time constraints in non-renal organ recovery | South Seas Ballroom A/B |