Organ procurement organization (OPO) organ donor recovery center impact on donor case times
Christine Radolovic1, Elizabeth Brown1, Sharon West1, Richard Hasz1.
1Gift of Life Donor Program, Philadelphia, PA, United States
Introduction: Several organ donor recovery centers managed by Organ Procurement Organizations (OPOs), sometimes in partnership with local transplant centers, have been established in the United States. These centers are designed to streamline specialized resources including personnel and facilities required for donor management and recovery of organs for transplantation. Cost and staff scheduling efficiencies have been documented, but there has been little examination of overall case times for donors managed and recovered in an organ donor recovery center versus a donor hospital. Examination of case times as a measure of efficiency is timely given that changes to the national allocation system have led to increases in case times. Median DBD donor case times, defined as the time from brain death pronouncement to donor cross-clamp, have, for example, increased nationally from 48.85 hours in 2020 to 55.97 hours in 2022.
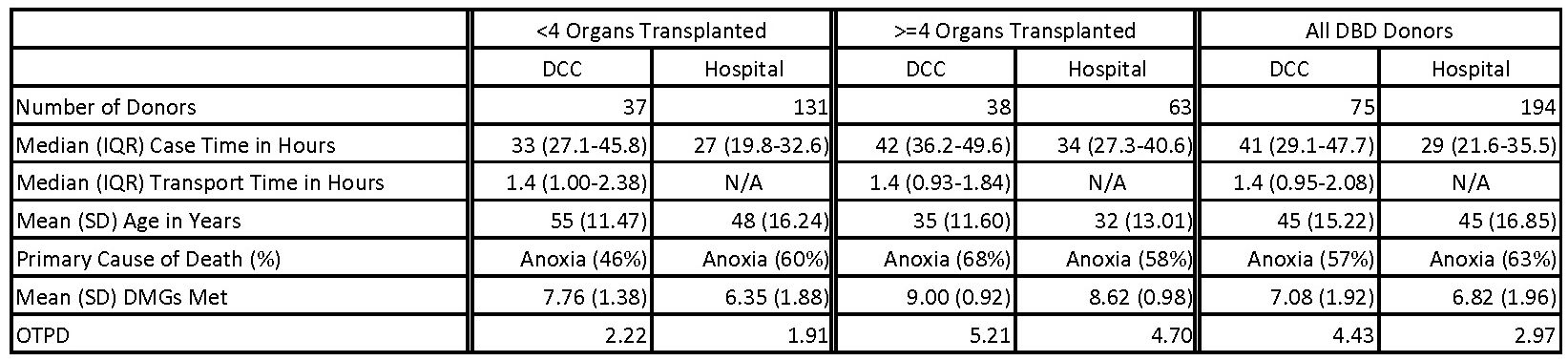
Method: This was a retrospective analysis of 269 DBD organ donors recovered by a single large OPO in the United States between September 2022 and April 2023. Some donors were transported to a centralized Donor Care Center (DCC), launched in September 2022 in partnership with a large transplant center, based on clinical assessment and referring hospital location following brain death pronouncement. Donor demographics and case times were compared between donors recovered at the DCC versus a donor hospital, and further evaluated based on whether fewer than or four or more organs were transplanted. The mean number of Donor Management Goals (DMGs) met out of ten was also compared across groups.
Results: Of the 269 DBD donors recovered, 75 (28%) were recovered at the DCC after being transferred from one of 38 referring hospitals and 194 (72%) were recovered at one of 75 donor hospitals in the OPO’s designated service area. Significantly longer case times were associated with donors recovered at the DCC (41 vs 29 hours, p<0.01). DCC case times were significantly longer both when there were fewer than four organs transplanted (33 vs 27 hours, p=0.016) and when there were four or more organs transplanted (42 vs 34 hours, p<0.01). Median transport time for donors from referring hospitals to the DCC was 1.4 hours. DCC donors with fewer than four organs transplanted were significantly older (55 vs 48 years, p=0.015) and met significantly more DMGs at time of recovery (7.76 vs 6.35, p<0.01).
Conclusion: In an increasingly complex national allocation system, OPOs must look for ways to optimize organ donation process efficiencies including case times. In its first six months of operation, case times were significantly longer when recovered at this DCC and could not be explained solely by transportation times added to these cases.
